1601006066
LONG CASE FINAL EXAM :
Hall ticket no - 1601006066
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
CASE :
A 65 year old male, resident of Veliminedu, Chityal who is a maestri by occupation 8 years back , came to the outpatient department on 12th of April 2021.
Chief complaints :
Swelling in both the legs since 14 days and altered sensorium since 2 days.
History of presenting illness:
The patient was apparently asymptomatic 14 days ago, he then developed swelling in both the legs which was insidious in onset, gradually progressive, grade 3 pitting oedema, aggravated on rest and relieved by walking. It was associated with facial puffiness which was noticeable early in the morning. History of decreased urine output since 10 days. Members of the family complained of abnormal behaviour such as inappropriate shouting since 2 days.
Not associated with nausea, vomiting, dyspnea, fatigue, abdominal pain, cough or palpitations.
Past history:
Similar complaints of pedal oedema and decreased urinary output were present 5 months ago. The patient took medication (Furosemide 10mg) prescribed by a local doctor and stopped the medication once the symptoms subsided.
He is a known case of hypertension since 12 years and is taking Metaprolol and Amlodipine since then.
Not a known case of diabetes mellitus, tuberculosis, asthma and seizures.
Personal history:
Diet: Mixed
Appetite: Decreased
Bowel and bladder: Regular
Sleep: Adequate
Addictions: None
Family history:
No significant family history.
Treatment history:
He has been put on dialysis since admission and has completed 6 sessions.
Torsemide 10 mg since 5 months.
General examination:
Patient is in altered sensorium while examining.
Temperature: Afebrile
Pulse rate: 82 bpm, regular in rhythm
Blood pressure: 140/80 mm of Hg
Respiratory rate: 16 cycles per min
Pupils: Bilateral reacting to light
Physical examination:
Pallor: present
Icterus: absent
Cyanosis: absent
Clubbing: absent
Oedema: absent
Lymphadenopathy: absent
Central nervous system examination:
GCS: E4V3M6
Motor system :
Right Left
Tone:
Upper limb - Normal Normal
Lower limb - Normal Normal
Reflexes:
Biceps - 2+ 2+
Supinator - 2+ 2+
Triceps - 2+ 2+
Knee - 2+ 2+
Ankle - 1+ 1+
Babinski - Negative Negative
• All superficial reflexes are intact.
• Sensory system and cranial nerves: not able to assess.
Per abdomen examination:
Umbilicus midline and inverted
Soft, non tender and no organomegaly
No shifting dullness or fluid thrill.
Bowel sounds are present.
Kidneys were not palpable bimanually.
CVS examination:
S1, S2 sounds are heard.
No murmurs, apex beat heard at left 5th ICS, medial to MCL.
Respiratory system examination:
Normal vesicular breath sounds heard.
Bilateral air entry present.
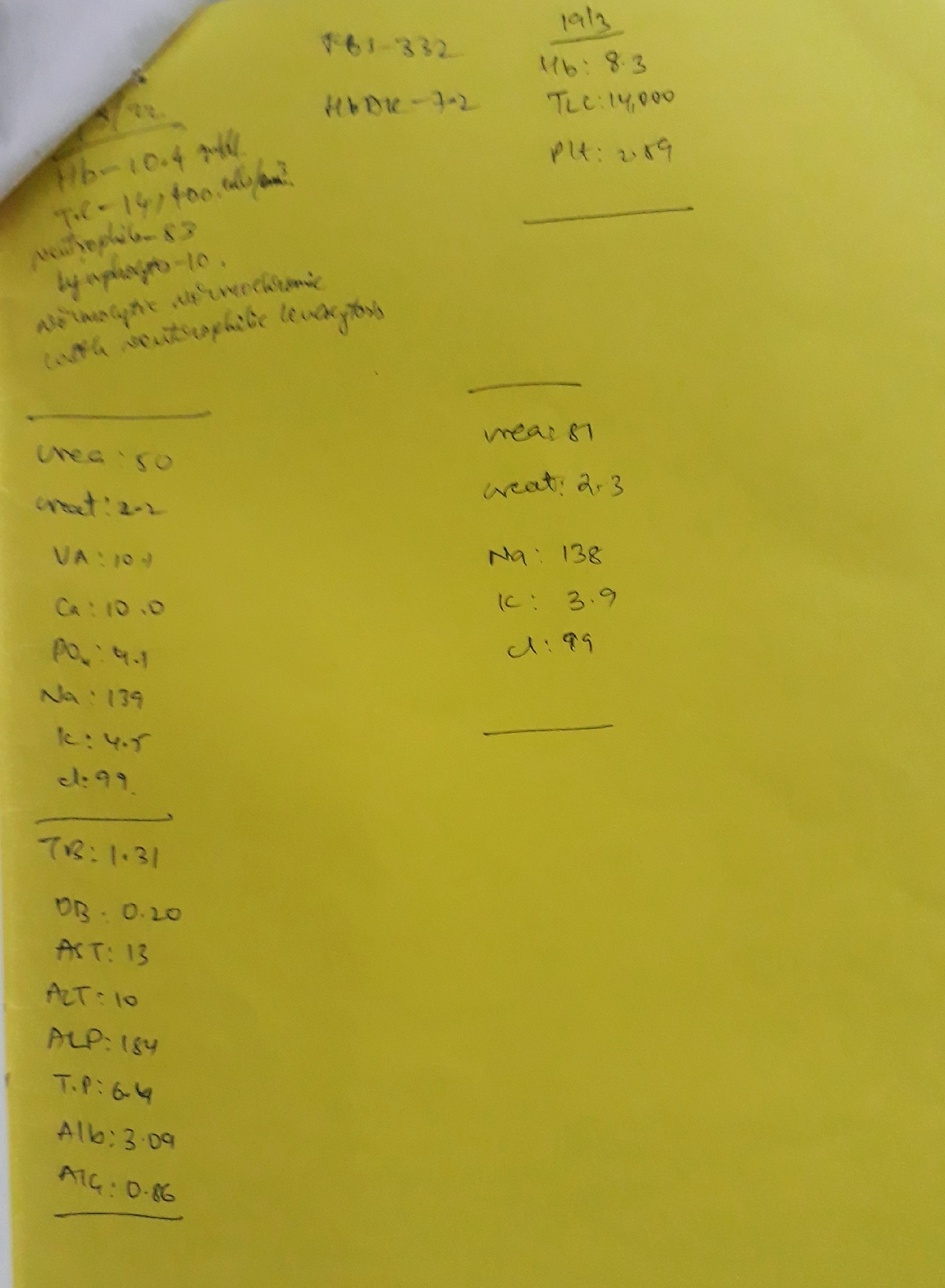
Investigations:
Complete Blood Picture :

Complete Urine Examination :

Ultrasound Abdomen :

Chest X - Ray :







Medication used :



Comments
Post a Comment